| SHOULDER JOINT |
 |
|
|
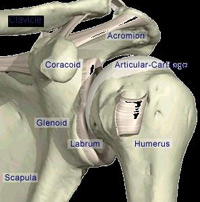
The shoulder is a very mobile joint capable of complex movements to enable us to achieve specific tasks. The shoulder has three components: the acromioclavicular joint, glenohumeral joint and the scapulothoracic articulation.
|
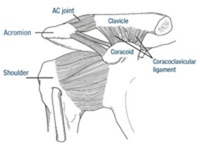 |
| Fig. 1 AC joint area anatomy |
|
1. Acromioclavicular or AC Joint
The area of interest lies just on top of the shoulder joint itself and involves the connection between the collar bone (clavicle) and a part of the shoulder blade called the acromion. The joint is held firmly in place by ligaments |
| |
| Structural damage and consequences |
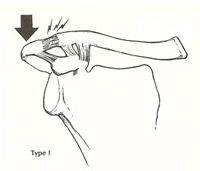
In a mild injury there is a simple sprain of the ligaments and capsule of the AC joint (Grade I),or a partial tearing of the ligaments allowing slight separation of the AC joint (Grade II). [See Fig 2 & 3]. |
These injuries result in pain and local swelling and in the case of Grade II injuries a permanent increase in the bump of the outer end of the collar bone.
Grade I and Grade II injuries can be treated in a sling for a few weeks to allow pain to settle and thereafter by a physiotherapy programme to ensure full movement of the shoulder is regained and to restore strength. |
| |
 |
 |
 |
Fig.2 Grade I |
Fig.3 Grade I |
Fig.4 Grade I |
|
| |
A severe AC joint injury involves complete rupture of both the AC joint ligaments and the coracoclavicular ligaments. This results in a wide separation of the AC joint with elevation of the collar bone and subsequently a prominent bump and change in contour of the shoulder (Grade III)
[See Fig. 4] Problems: |
- persistent pain in the area
- clicking or catching with movement of the shoulder in certain positions
- reduction of full strength in the arm and restriction in the ability to carry out activities or work place duties where there is a requirement to frequently lift or manoeuvre objects at or above the shoulder height.
|
| |
| Treatment |
Grade III AC separation can be treated with Surgical treatment. Surgery is much more successful for Grade III AC separations when performed early
(within 2 to 3 weeks of the injury). When done early the surgery is less complicated and results in the natural healing of the coracoclavicular ligaments rather than requiring a graft. |
| It is recommended to consider having the surgery performed early after the injury in people who engage in throwing or contact sports or those who perform overhead or heavy manual work. |
| |
| 2. Glenohumeral Joint |
|
The main part of the shoulder consists of the ball at the top of the arm (humerus) which sits in a shallow socket (glenoid) connected to the shoulder blade (scapula). The socket has a ring of cartilage (labrum) around its edge which deepens it and helps keep the ball in it. Surrounding the shoulder joint is a watertight sac called the joint capsule. The joint capsule holds in fluids that lubricate the joint. The walls of this capsule are made up of ligaments. These ligaments loosely connect the ball to the socket and attach to the ring of cartilage (labrum) at its edge. They become tight if the shoulder rotates too far in any direction and prevent the ball slipping out of the socket (a dislocation). One of the biceps tendons enters the shoulder and attaches to the ring of cartilage near the top of the socket. |
| |
| Structural damage |
| Shoulder Instability most commonly occurs due to separation of the ring of cartilage (the labrum) plus the capsule and shoulder ligaments attached to it from the bone of the shoulder socket (referred to as a Bankart injury or tear). Usually this is created by a complete dislocation of the shoulder. It may, however, result from an injury where the shoulder is stretched or wrenched in an abnormal direction but without actually dislocating. |
| |
| Consequences |
| The Bankart injury results in instability of the shoulder which can lead to: |
- Repeated dislocations of the shoulder - the younger the age at first dislocation, the greater the chance of experiencing another
- Feelings of looseness in the shoulder with the arm in certain positions or with certain activities
- Lack of strength or confidence in the arm
- Pain or clicking with the shoulder in certain positions (SLAP tear)
- Arthritis of the shoulder if present for many years
|
| |
| Treatment |
| Research indicates that early surgical repair following a dislocation of the shoulder will result in less chance of dislocation later, as well as less looseness and more confidence in the arm. It is for this reason that surgical repair is now offered as a treatment option for a first dislocation in young people and professional athletes. The success of the surgery performed at this stage is higher than that following many months or years of shoulder instability and often numerous dislocations. |
| There is some evidence to show that the duration of instability and the number of dislocations relates to the long-term prognosis of the shoulder, particularly with respect to the development of arthritis. |
| |
| The Surgery |
|
|
Stabilisation surgery (shoulder 'reconstruction') is performed under general anaesthetic and usually via a keyhole (Arthroscopic) technique. |
|
| |
| Shoulder Arthroscopy |
| 2 or 3 small incisions ( 1 cm each) are made around the shoulder through which the camera (arthroscope) and plastic instrument tubes are inserted |
| |
 |
 |
Bankart tear |
Bankart tear - repair |
|
| |
|
| |
The cartilage is repaired and the ligaments in front of the shoulder tightened with small (2.3/2.5mm) suture-Anchors. Pictures or video of the operation can be taken during the procedure.
The keyhole technique has some advantages compared with traditional methods of 'open' surgery using larger incisions: |
- Less pain
- Shorter hospital stay (day case or overnight only)
- Faster rehabilitation
- Less stiffness (restriction of movement) following the surgery
- Better ability to identify and treat other areas of damage
|
| |
| SLAP Tears |
SLAP tears are separations of cartilage from bone inside the shoulder from 10 to 2 o clock position, which cause pain, clicking or feelings of looseness of the shoulder. They may arise after a single traumatic event such as a fall onto the shoulder or attempt to lift a heavy object, or through repetitive overhead or throwing sports or work duties. They can also exist alongside other cartilage and ligament damage following a shoulder dislocation. |
The biceps tendon itself may separate from the bone along with the cartilage. The tear can extend further along the rim of the socket down the front or the back, and multiple tears within the labrum itself can occur. |
| |
| Consequences |
| The SLAP lesion can result in: |
- Pain in the shoulder
- Reduced performance with overhead or throwing sports
- Catching or clunking with movement
- "dead-arm" sensations
|
| |
| Treatment |
SLAP tears do not generally heal by themselves; however, may become less symptomatic with time.
Initial treatment after a traumatic event may involve use of a sling for a short period plus analgesics. Later, avoiding the position of the arm or activity which reproduces the pain will help but may not be possible or desired. Physiotherapy can help to restore movement initially and regain strength after a period of decreased use of the arm, but cannot help to heal the structural defect in the cartilage.
Surgical repair is indicated when symptoms do not settle down adequately with time, or in some cases will be advised earlier depending on the exact type and size of SLAP tear present. If the SLAP tear is present along with other tearing (e.g. a Bankart tear) following a dislocation, then surgery will very often be required. |
| |
| Surgery-Shoulder Arthroscopy |
| |
 |
 |
SLAP tear |
SLAP tear after repair |
|
| |
Stitches are passed through the torn labrum and the biceps tendon and secured to the bone with small anchors, the aim being to encourage the labrum and tendon to heal down strongly to the bone. |
| |