| KNEE JOINT |
 |
|
|
The knee is a synovial joint, which provides a stable support for the body and enables a person to ambulate. Both flexibility and stability are needed for standing, walking, running, crouching, jumping, and turning.
Fixed and moving parts, including bones, cartilage, muscles, Menisci, ligaments, and tendons, enable the knee to function normally. Any disruption to these structures results in dysfunction and pain and swelling are the most common symptoms.
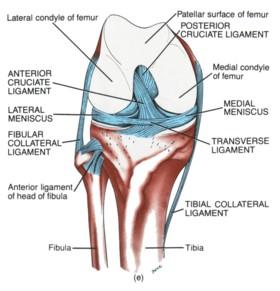
Bones and Cartilage: Thigh bone"Femur" and Leg bone"Tibia" forms the Joint. Knee Cap"Patella" is the small bone in extensor mechanism and important for strength and stability of Joint. Cartilage is the smooth white layer that you see on the end of a lamb or chicken bone where it forms a joint. Cartilage is extremely important for smooth joint function and lubrication.
|
|
Muscles: The quadriceps muscle comprises of four muscles on the front of the thigh that work to straighten the leg from a bent position. The hamstring muscles, which bend the leg at the knee, run along the back of the thigh from the hip to just below the knee. Keeping these muscles in good condition will help prevent knee injuries as the muscle can absorb a significant amount of load.
|
Ligaments: The medial collateral ligament (MCL) provides stability to the inner (medial) part of the knee.
The lateral collateral ligament (LCL) provides stability to the outer (lateral) part of the knee.
The anterior cruciate ligament (ACL), in the center of the knee, limits rotation and the forward movement of the tibia.
The posterior cruciate ligament (PCL), also in the center of the knee, limits backward movement of the tibia.
Other ligaments are part of the knee capsule, which is a protective, fiber-like structure that wraps around the knee joint. Inside the capsule, the joint is lined with a thin, soft tissue called synovium. |
| Menisci: These are two half-moon shaped structures that sit on the top of the tibia. The menisci act as a Shock absorbers, Nutrition supplier, Joint protector and Stabilizing structure. They are most commonly injured when the knee suddenly twist as in a sporting accident. |
| |
| Knee Arthroscopy |
Arthroscopy of the knee is usually performed to diagnose and treat internal knee problems such as cartilage injuries, meniscal tears, loose bodies, arthritis and a lead up for ligament damage surgery. Arthroscopy is a "key-hole" Surgery in which 2.4-4mm size tiny Fibre optic Telescope is inserted into the joint which is then attached to Camera to visualize on TV Monitor. Simple arthroscopy procedures are carried out in hospital as a Day Case. But in case of Ligament Reconstruction/Repair (ACL, PCL, MCL, LCL) you may require an overnight stay. |
|
| |
|
| |
| What to Expect when having a Knee Arthroscopy |
On the day of your surgery, you will initially meet the nursing staff in the Day Care Unit and have a brief check up by your anaesthetist. Your knee will then be prepared with hair removal and a wash. From the Day Care Unit you will be taken to the operating theatre to meet Dr. Sonar prior to your surgery. In most cases, the knee arthroscopic procedure will be carried out under a Spinal anaesthesia. |
 |
 |
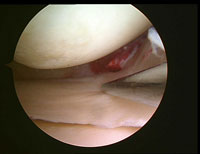
| Meniscus Tear |
|
| |
| Knee Arthroscopy Surgery - Outline of the Procedure |
Your knee will be washed with antiseptic solution and a tourniquet applied to the thigh to prevent bleeding during the operation.
The arthroscope is introduced into the knee through a small puncture wound beside the knee cap. Initially a thorough examination is made of the entire knee and then particular reference is made to the problem as discussed with you by Dr. Sonar |
 |
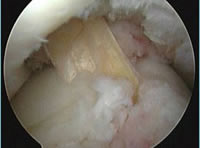 |
| ACL Reconstruction |
|
Cartilage damage, loose bodies, Ligaments and arthritis are then treated with small instruments that may be introduced through a second puncture wound on the other side of the knee cap. Photos are taken of your knee during your procedure.
At the end of the operation, the small puncture wounds will be closed with steri strips (an occasionally with sutures), the knee is then wrapped up with a sterile bandage. |
|
Recovery
After the surgery, you will then be taken to the recovery room and eventually back to the Day Care Unit. You will be given an instruction sheet outlining your post operative care and also a photo of your knee taken during the procedure. Detailed findings of your surgery will be given to you at your post operative appointment which will be made for you approximately 10 days following the surgery.
Discharge from Hospital
You will be required to stay in hospital for at least 2-3 hours following your procedure before you will be discharged
You must have someone available to drive you home from hospital.
You must not operate machinery or drive a car for 24 hours after your procedure.
You should have a responsible adult with you at home for at least the first 24 hours.
Post Operative Appointment
It is important that you attend this appointment usually 10 days post operative, as part of your ongoing treatment/management.
You will be required to rest completely for the first 2-3 days following surgery. This means Sitting in bed or on the couch, doing some light exercises and icing the knee regularly. By the 3th or 4th day you may start to walk around a little. If you work in an office you may then return to work. More active jobs may require longer periods off work e.g. up to 2-3 weeks for manual labourers. |
Physiotherapy and Rehabilitation:
Theme: Rest. Swelling, bruising control. Pain control
Week 0 - 2 (approximate)
- The aim of this stage is to recover after surgery. You should spend the time at home resting. Stay mainly on the couch. Wear your Brace.
- Take pain killers as required. Stay well hydrated.
- Icing: Ice your knee for 30mins: 5 or 6 times a day.
- Use crutches but weight bear as tolerated
- Try to lock your knee out straight and tighten the quadriceps
- Pump the calf muscles every chance you get
|
Rehabilitation Phase 1
Theme: Range of Movement (ROM)
Week 2-6 (approximate)
- The main aim here is to achieve a good ROM. Most importantly complete extension (knee out straight equal to the opposite healthy knee). Practice your knee extension locking exercise (most important), knee bending and prone hanging. Ask your physiotherapist or Dr. Sonar for details
- You should attempt to achieve a normal walking style
- You may commence stationary cycling when comfortable
- Resume normal daily activities
- Continue icing the knee
- This phase usually lasts about 6 weeks but may vary between 3 and 12 for example.
- Sometimes you will be told to slow down or speed up
- You will have regular reviews with Dr. Sonar and your physiotherapist.
- GOALS: A good ROM, complete extension, no swelling
- If you achieve all the desired goals you may move on to the next phase of rehabilitation.
|
Rehabilitation Phase 2
Theme: Strength, balance
Week 6 - 12 (approximate)
- This phase usually lasts about 6 weeks, but may vary between 3 and 12 for example
- You should now be walking normally and performing normal activities of daily living
- It is now time to commence a gym based programme emphasising strength of all muscle groups including quadriceps, hamstrings, calf, gluteals, core strength. Balance exercises are also important
- Activities include walking, cycling, swimming (no breaststroke), rowing
- Don't over do it. Ice after activity
- GOALS: Normal gait, swimming, cycling, one leg squat to 90°
- If you achieve all the desired goals you may move on to the next phase of rehabilitation
|
|
Rehabilitation Phase 3
Theme: Light agilities
Week 12 - 20
- You may now commence jogging (if given the all clear)
- Plyometrics begin - hopping, jumping, etc
- Zig zag running
- Don't overdo it
- Ice after activities
|
Rehabilitation Phase 4
Theme: More aggressive agility exercises
Week 20+
- Sport specific exercises. Refer to Dr. Sonar and your sport physiotherapist
- Endurance
|
Once you have completed Phase 4 you have essentially completed your rehabilitation. We do however, need to know that you have achieved a state of recovery good enough to protect your "new" knee. We have developed a score that accurately predicts whether or not you have attained a full recovery after your injury and surgery. |
| |